
Diseases/Conditions
Current Status of Aluminum Adjuvant Research: Focus on Autism

The focus on this page of the Keele Conference article is on the status of scientific studies on aluminum adjuvants in relation to autism spectrum disorders. The results are compelling. The question is: Do they meet the scientific standard of proving cause-and-effect?

Syringe Dripping Aluminum Balls. (Aluminum balls clipped from photo by CG Hughes, with skull & crossbones added. Word Autism added to background.)
by Heidi Stevenson
Continued from Page 1
Dr. Shaw continued his talk with a focus on autism and the status of research into aluminum adjuvants and their relation to it and other neurological disorders.
Aluminum in Vaccines and Autism Spectrum Disorder (ASD)
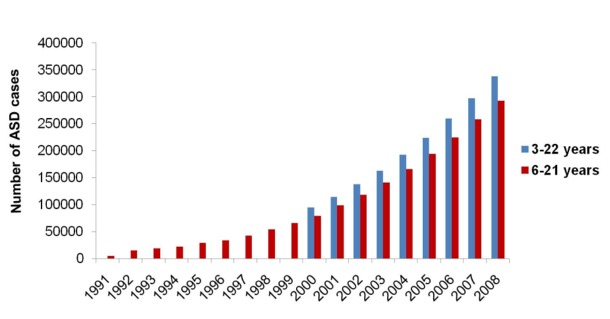
Shaw stated that autism is a severe condition that involves “dysfunctions in language, social interactions, and general immune responses.” There has been a dramatic increase since the 1990s. Hypotheses for this increase include gene shift, changed diagnostic criteria, more general awareness, population increase, toxins, and gene-toxin interactions, among others less well known.
The prevalence of ASD since 1990 is clearly demonstrated by this graph:
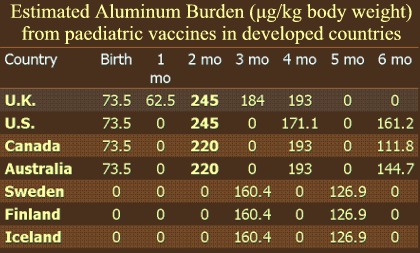 The chart to the right displays, by country, the aluminum (Al) burden placed on children via vaccines during their first six months of life.
The chart to the right displays, by country, the aluminum (Al) burden placed on children via vaccines during their first six months of life.
In a 2011 study, Shaw and his team documented an exceptionally strong correlation between exposure from Al adjuvants and the number of ASD cases. They used the statistical analysis called the Pearson correlation, which is presented in the next graph.

Pearson Correlation of ASD with Aluminum in Vaccines
The calculation, done 3 times, accounts for small, medium, and high exposures to Al in vaccines. Each graph point represents the number of ASD cases recorded in that year. The three steeply-sloping lines show the Pearson correlation-defined relationship, which was calculated at 0.92, which is exceptionally high and strongly indicative of an association between Al in vaccines and ASD.
This study’s analysis also found that :
- Al adjuvant exposure correlates with age of exposure.
- Countries with greater Al-adjuvanted vaccine schedules have higher ASD rates.
- The US, UK, and Canada have the highest ASD rates in so-called “western” countries, while the rate is lower in Nordic countries.
- Eight of the nine Hill’s criteria are satisfied by the evidence.
Hill’s criteria are a group of questions that should be satisfied to demonstrate a cause and effect association in diseases. These are:
- Strength of data,
- Consistency of data/results,
- Biological plausibility. Is there a reasonable explanation for how the potential causes induce the disease?
- Temporal relationship, which is shown in the Peason correlation.
- Biological gradient. Is greater exposure associated with worse disease?
- Coherence. Does the potential cause result in other, related biological effects?
- Experimental evidence.
- Analogy with similar evidence.
- Specificity. This criterion is not necessarily relevant to ASD because it may have multiple causative factors.
You can read more about this study and this analysis, along with a larger, easier-to-read Pearson correlation graphic and the Hill criteria, here.
Animal Studies in Aluminum Adjuvants
Before discussing the work on aluminum vaccine adjuvants in animal research, he reviewed some caveats:
- The formulation of Al used in experiments may differ from commercial formulations.
- Different Al adjuvants may have different impacts.
- Mouse to human age comparisons are problematic.
- There is a wide range of behavioral studies that could be done.
Nonetheless, animal studies have provided significant data that ties Al adjuvants to ASD. The following graphs all demonstrate the results of an experiment that examined behavior in male and female mice after injection with an Al adjuvant. These mice were not specially bred, thus their behavior is likely to vary. That helps make a more legitimate comparison between mouse and human behavior.
Behaviorial Effects
The graphs below refer to experiments performed on mice that, as closely as possible, were injected with adjuvants (or a placebo) to match the equivalent human ages from birth to age six. “Low alum” refers to the amount of aluminum in vaccination schedules of Scandinavian countries. “High alum” refers to the amount of aluminum in vaccination schedules of the US and UK.
The first two graphs refer to experiments involving light boxes, in which mice could move to dark or light areas. Results of males are shown on the left and females to the right. What is clearly shown here is that the mice behave differently after Al injection, and that the responses vary between males and females.
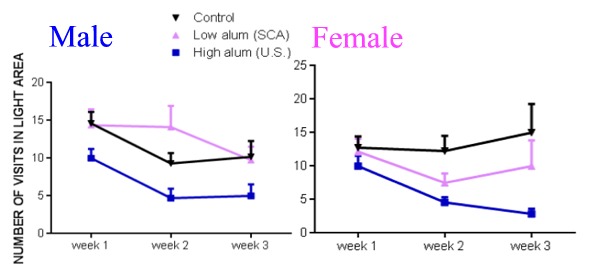 In the first graph, it’s clear that males tend to be more exploratory initially after injection with a low dose (week 2), but then tend to lose that trait (week 3). High dose Al, though, results in less exploratory behavior immediately and it keeps getting worse. Females become less exploratory with both low and high doses.
In the first graph, it’s clear that males tend to be more exploratory initially after injection with a low dose (week 2), but then tend to lose that trait (week 3). High dose Al, though, results in less exploratory behavior immediately and it keeps getting worse. Females become less exploratory with both low and high doses.
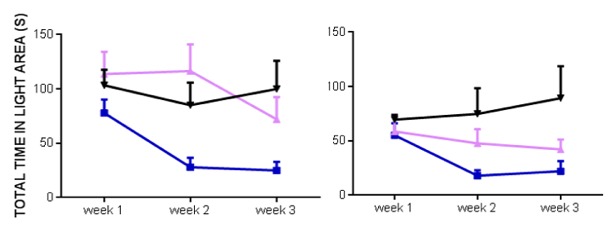 Expressed in time spent in light areas, instead of instances of entry, we can see a similar pattern. Therefore, mice not only enter light areas more often, they also tend to stay there.
Expressed in time spent in light areas, instead of instances of entry, we can see a similar pattern. Therefore, mice not only enter light areas more often, they also tend to stay there.
When placed in a cage that allows freedom of movement, differences in how frequently the mice rear and move from seemingly safer areas to more open ones is demonstrated. Injection with Al adjuvants causes a significant change in behavior, again with distinctions between males and females, as demonstrated by the next two graphs:
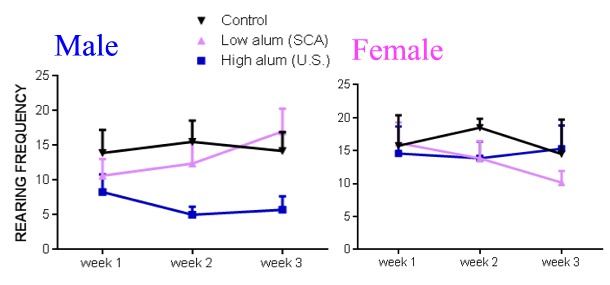 Rearing is indicative of a mouse’s exploratory behavior. Injection with Al adjuvants causes a significant change in frequency of rearing, again with distinctions between males and females. As you can see, at weeks 1 and 2, males injected with low Al doses demonstrate less inclination to rear than the controls, but that tendency reverses by week 3. However, high dose Al results in dramatic lessening of this behavior. Females tend to show a milder response.
Rearing is indicative of a mouse’s exploratory behavior. Injection with Al adjuvants causes a significant change in frequency of rearing, again with distinctions between males and females. As you can see, at weeks 1 and 2, males injected with low Al doses demonstrate less inclination to rear than the controls, but that tendency reverses by week 3. However, high dose Al results in dramatic lessening of this behavior. Females tend to show a milder response.
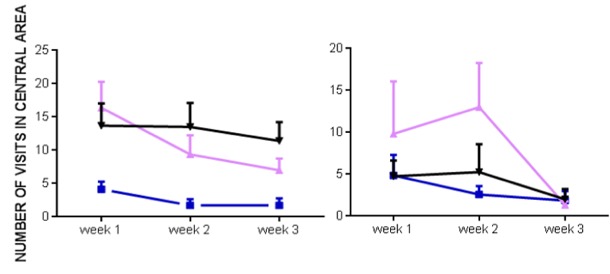 In terms of the number of visits made to the central, open area of the cage. it’s clear that high doses of Al almost completely end that behavior in males with high dose Al. In females, the story is quite different. With low dose Al, their central area visits are dramatically increased in weeks 1 and 2, but then plummet in week 3. However, their behavior is not much different with high dose Al.
In terms of the number of visits made to the central, open area of the cage. it’s clear that high doses of Al almost completely end that behavior in males with high dose Al. In females, the story is quite different. With low dose Al, their central area visits are dramatically increased in weeks 1 and 2, but then plummet in week 3. However, their behavior is not much different with high dose Al.
Physiological Changes
The following graph shows the the effect on mouse weight that results after Al has been injected. (Please note that the scales are different because male mice tend to be larger than females.)
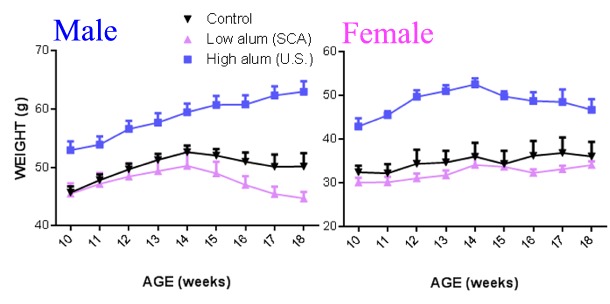
It appears that both male and female mice given low-dose Al injections end up weighing less and staying that way. However, high-dose injections have the opposite effect, and dramatically so, on both sexes.
Dr. Shaw also highlighted research showing immunohistological research showing that aluminum is associated with effects on animal biology. IBA-1 is a protein shown to be activated in microglia, indicating nerve damage. T-cells labeled by CD3 antibodies have been found in the hippocampus region of the brain, indicative of an inflammatory, possibly autoimmune, response activated by aluminum.
Increases in GFAP (glial fibrillary acidic protein) indicate neural processes that lead to neurodegeneration. Aluminum adjuvants have been shown to be associated with this process.
Conclusions
Dr. Shaw pointed out that:
- Aluminum is toxic in living animals.
- Aluminum in vaccines has been correlated to ASD in an “ecological” study. It is both statistically significant and satisfies all but one of Hill’s criteria.
- Mice given aluminum equivalent to a current pediatric schedule suggest that its impacts are dose-dependent.
- Histological changes include neuroinflammatory responses in both male and female mice.
- Some of these responses may be caused by an autoimmune reaction. They may, therefore, be part of the ASIA (autoimmune inflammatory) syndrome associated with adjuvants.
Where from Here?
Dr. Shaw’s lab, Neural Dynamics Research Group, works in conjunction with collaborators at the Gherardi lab in France. They are working on sorting out effects of different aluminum compounds, routes of access to parts of the body, age-related effects, varieties of effects, and other related issues. These include:
- Longitudinal studies.
- Identification of susceptibility genes and single nucleotide polymorphisms (SNPs – small sections of DNA). It should be noted here that Dr. Shaw is not suggesting that there’s a genetic cause of autism, that it is, in fact, ludicrous to suggest it. The research he recommends is on genetic changes associated with Al adjuvants.
- Gene-toxin interactions should be explored.
- Synergies between toxins need to be investigated. For example, mercury has been implicated in autism. What, if any, interaction between mercury and aluminum might explain it? Does that interaction ease, worsen, or change the effects?
- Investigation of potential generational effects from epigenetics, that is, changes to the gene that are passed on to succeeding generations.
Dr. Shaw also suggests:
- Imaging studies in humans to find out where aluminum goes and how long it lasts in the central nervous system.
- Studies into removal of aluminum from the central nervous system.
Clearly, the science on cause and effect is not complete on aluminum’s effects in vaccines. Dr. Shaw is quite specific about that. However, my observations of the response to his talk by the other scientists in the room was informative. He wasn’t questioned on the legitimacy of his research or critiqued on flaws in the studies. The questions centered around how to replace aluminum in vaccines.
The majority of scientists at the Keele Conference were in favor of vaccination, some even vehemently so. Afterwards, I debated the issue of vaccination in general with a couple of the scientists who asked Dr. Shaw about alternatives, but were strongly in favor of vaccinations. Nonetheless, they were impressed with his evidence, and they seemed to believe that we should be discussing the removal of aluminum from vaccines. Clearly, they believed his evidence is strong—enough to be interested in moving beyond discussion of whether it’s a risk, but instead discussing how to replace it.
The question becomes, at what point do you decide that the evidence is strong enough to support elimination of aluminum from vaccines? Do we truly need absolute proof before removing something that we know to be harmful in general, that epidemiological evidence clearly shows is associated with harm, and for which a means of causing such harms has been shown? All these factors have been shown to be true of aluminum adjuvants. At what point is the evidence strong enough?
Sources:
- Administration of aluminium in vaccine-relevant exposures in neonatal mice is associated with long-term adverse neurological outcomes, page 61 of Keele Conference abstracts.
Sources referenced by Shaw in his talk:
- Some Objections to the Use of Alum Baking Powder, JAMA; William J. Gies, Ph.D; doi:10.1001/jama.1911.04260090038015
- Aluminum Vaccine Adjuvants: Are They Safe?, Journal of Inorganic Biochemisty; L. Tomljenovic and C.A. Shaw; doi:10.1016/j.jinorgbio.2009.05.019.
- Aluminum hydroxide injections lead to motor deficits and motor neuron degeneration; Journal of Inorganic Biochemisty; Christopher A. Shaw and Michael S. Petrik; 10.1016/j.jinorgbio.2009.05.019
- Aluminum Adjuvant Linked to Gulf War Illness Induces Motor Neuron Death in Mice; Neuromolecular Medicine. 2007;9(1):83-100; Petrik MS, Wong MC, Tabata RC, Garry RF, Shaw CA
- Aluminum-based adjuvants should not be used as placebos in clinical trials, Vaccine; Exley, C; doi: 10.1016/j.vaccine.2011.08.062
- A role for the body burden of aluminium in vaccine-associated macrophagic myofasciitis and chronic fatigue syndrome; Medical Hypotheses; Exley C, Swarbrick L, Gherardi RK, Authier FJ; doi: 10.1016/j.mehy
- ‘ASIA’—Autoimmune/inflammatory syndrome induced by adjuvants, Journal of Autoimmunity; Shoenfeld Y, Agmon-Levin N.; doi: 10.1016/j.jaut.2010.07.003
- Long-term persistence of vaccine-derived aluminum hydroxide is associated with chronic cognitive dysfunction, Journal of Inorganic Biochemistry; Couette M, Boisse MF, Maison P, Brugieres P, Cesaro P, Chevalier X, Gherardi RK, Bachoud-Levi AC, Authier FJ; doi: 10.1016/j.jinorgbio.2009.08.005
- Do aluminum vaccine adjuvants contribute to the rising prevalence of autism? Journal of Inorganic Biochemistry; Lucija Tomljenovic and Christopher A. Shaw; doi:10.1016/j.jinorgbio.2011.08.008
- Empirical Data Confirm Autism Symptoms Linked to Aluminum and Acetaminophen Exposure, Journal of Inorganic Biochemistry; Stephanie Seneff, Robert M. Davidson, and Jingjing Liu; doi:10.3390/e14112227
- Mechanisms of aluminum adjuvant toxicity and autoimmunity in pediatric populations; Journal of Inorganic Biology; Tomljenovic, L, Shaw, CA; doi: 10.1177/0961203311430221
- Autoimmunity following Hepatitis B vaccine as part of the spectrum of ‘Autoimmun (Auto-inflammatory) Syndrom induced by Adjuvants’ (ASIA): analysis of 93 cases, Lupus; Zafrir Y, Agmon-Levin N, Paz Z, Shilton T, Shoenfeld Y; doi: 10.1177/0961203311429318
- Autism spectrum disorders and aluminium vaccine adjuvants, The Comprehensive Guide to Autism, Springer Reference; Dr. Lucija Tomljenovic, Professor Russell L. Blaylock, Dr. Christopher A. Shaw
- Do aluminum vaccine adjuvants contribute to the rising prevalence of autism? Journal of Inorganic Biochemistry; Tomljenovic L., Shaw CA; doi: 10.1016/j.jinorgbio.2011.08.008
- Empirical Data Confirm Autism Symptoms Related to Aluminum and Acetaminophen Exposure; Entropy; Stephanie Seneff, Robert M. Davidson, Jingjing Liu; doi:10.3390/e14112227
- Mechanisms of aluminum adjuvant toxicity and autoimmunity in pediatric populations; Lupus; Tomljenovic L., Shaw CA; doi: 10.1177/0961203311430221
Tagged aluminum adjuvant, aluminum adjuvant research, aluminum adverse effects, aluminum asd, aluminum autism, aluminum autism spectrum disorder, aluminum in vivo data, aluminum keele meeting, aluminum neurological effects, aluminum neurotoxin, aluminum pediatric vaccines, autism, autism and aluminum adjuvants, autism vaccines, ca shaw research, chris shaw aluminum, keele conference, science, vaccine, vaccines, wire mesh hang experiment












Pingback: Current Status of Aluminum Adjuvant ResearchGaia Health